Every LDCT lung cancer screening scan captures coronary artery data that, until now, has largely gone unreported and unreimbursed.
Effective
April 1, 2026, CMS established
HCPCS code G0680 — a dedicated reimbursement pathway for algorithmic analysis of coronary artery calcium (CAC) and aortic valve calcification (AVC) from chest CT. G0680 is assigned to APC 1492 (New Technology APC) under OPPS, with a national unadjusted rate of approximately $15.50 per case (subject to local wage index adjustments per CMS Addendum B).
The code's strategic significance, however, lies not in the line-item rate but in the downstream clinical and economic pathway it activates. A single $15.50 analysis identifies high-risk patients who then enter workflows reimbursed at materially higher rates: CPT 75574 (CCTA) at ~$357 and CPT 75577 (AI-based plaque analysis, Category I as of January 2026) at ~$950–$1,000.This update marks the first time CMS has formally recognized AI-enabled opportunistic cardiovascular screening from routine chest CT as a billable service. For radiology practices and health systems already running lung cancer screening programs, this is a significant inflection point.
What G0680 Covers — and What It Requires
G0680 applies to algorithmic analysis of CAC and/or AVC from chest CT with report, in the hospital outpatient setting under Medicare. The key phrase is "from chest CT" — meaning any chest CT where AI-based analysis is performed, not exclusively LDCT lung cancer screening.
A few important scope details:
- No additional imaging required: G0680 is a post-processing service applied to already-acquired CT images. No new scan or additional radiation is involved.
- FDA clearance is required: The algorithm used must have appropriate FDA clearance for the intended use, such as K243696 for AVIEW CAC on non-contrast, non-gated chest CT including LDCT.
- Setting limitation: G0680 is currently established under OPPS for the hospital outpatient setting. Physician office and freestanding center reimbursement pathways have not yet been separately established.
- Coverage and Necessity: Code assignment does not guarantee payment. Actual reimbursement requires medical necessity documentation and satisfaction of the applicable MAC's "reasonable and necessary" standard.
Three Strategic Implications for the Field
1. Institutional Recognition of AI-Based Chest CT Analysis
Prior to G0680, software-based CAC analysis existed in a billing gray zone. With this code, CMS has formally recognized algorithmic image analysis as a
standalone reimbursable medical service, distinct from the underlying CT acquisition or the standard radiology read.
2. Enabling Monetization of Opportunistic Analysis
The primary value of G0680 is the
patient identification funnel it enables. The
AHA 2025 Scientific Statement estimates that more than
17 million eligible individuals undergo chest CT annually in the U.S., many of whom leave the encounter without their cardiovascular risk being identified.
What happens when these findings are reported? The
NOTIFY-1 project demonstrated that opportunistic AI-based CAC screening, followed by systematic clinician notification, led to a
statin prescription rate of 51.2% in the notification arm versus just 6.9% with usual care (Sandhu et al.). Once high-risk patients are referred, the downstream clinical pathway unlocks higher reimbursement:
- CPT 75574 (Coronary CT Angiography): ~$357
- CPT 75577 (AI-based plaque analysis, Category I as of Jan 2026): ~$950–$1,000
3. Validation of the Multi-Disease Chest CT Strategy
G0680 formalizes a "Multi-disease" workflow. A single chest CT (e.g., LDCT) now covers lung disease assessment plus cardiovascular risk evaluation (CAC, AVC) under G0680. This allows health systems to generate additional recognized clinical and economic value from the same imaging infrastructure already in place.
The Operational Reality: Manual CAC Analysis Doesn't Scale
Manual CAC analysis takes
5–10 minutes per case and introduces significant inter-reader variability. In high-volume screening environments, this burden is unsustainable. This is the exact problem that AI-powered analysis solves.
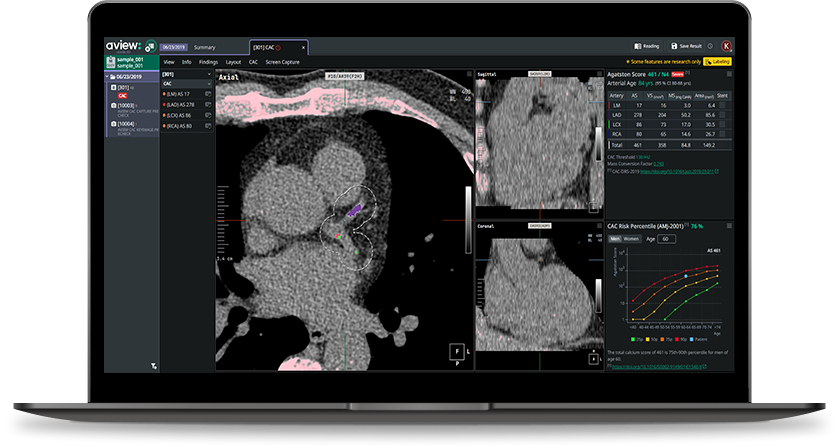
Coreline Soft's aview CAC
What an AI-Ready Workflow Looks Like: aview CAC
Coreline Soft’s aview CAC is specifically designed for this opportunistic environment:
- Kernel conversion: Automatically converts sharp kernel images (LCS standard) to soft kernel equivalents for accurate Agatston scoring.
- Anatomical segmentation: Segments the four major coronary arteries (LM, LAD, LCX, RCA) to reduce false positives from aortic or valvular calcification—a patent-protected methodology.
- Zero-click integration: Analysis runs automatically in the background. By the time a radiologist opens the viewer, results are already waiting.
Clinical Validation at Scale
- Accuracy: Agatston score agreement with ECG-gated cardiac CT reaches an ICC of 0.989.
- Prognostic Value (K-LUCAS): AVIEW CAC identified a higher CAC prevalence than visual assessment (60.1% vs. 53.4%). Patients in the "Severe" category had a 9-fold higher incidence of MACE than the "None" group (Park et al.).
- National Scale Validation: The Hagopian et al. (NEJM AI 2025) study validated AI-CAC algorithms across 98 VA centers, confirming that automated CAC detection is technically feasible and highly predictive of mortality at a national scale (Hagopian et al.).
What Practices Should Be Doing Now
G0680 is live. With CMS now recognizing AI-based CAC analysis as a distinct clinical service, every chest CT processed without it represents a missed opportunity to identify patients at cardiovascular risk. Assess these three areas:
1. Reporting consistency: Are CAC findings consistently reported across all chest CT scans?
: If not, AI-supported analysis can help standardize detection and reporting, supporting more consistent clinical documentation.
2. Workflow integration: Can CAC analysis be performed at scale without impacting radiologist workload?
: If not, integrated solutions can enable background processing that fits within existing clinical workflows.
3. Cardiology referral pathway: Are high-risk findings linked to a clear and actionable follow-up pathway?
: If not, structured reporting frameworks such as CAC-DRS can support more standardized communication and facilitate appropriate clinical follow-up.
Works Cited
• American Heart Association. “Opportunistic Detection of Cardiovascular Disease Risk on Non-Cardiac Computed Tomography: A Scientific Statement from the American Heart Association.” Circulation, vol. 151, 2025. https://doi.org/10.1161/CIR.0000000000001382.
• Centers for Medicare & Medicaid Services. “April 2026 Update of the Hospital Outpatient Prospective Payment System (OPPS).” Medicare Claims Processing Manual, Transmittal 13702CP, 2026.
• Hagopian, Robert, et al. “Deep Learning for Opportunistic Calcium Scoring in Low-Dose CT Lung Cancer Screening.” NEJM AI, vol. 2, no. 1, 2025. https://doi.org/10.1056/AIoa2400937.
• Park, Chansik, et al. “Prognostic Value of Automated Coronary Artery Calcium Scoring on Lung Cancer Screening Low-Dose CT: The K-LUCAS Study.” American Journal of Roentgenology, vol. 222, 2024.
• Sandhu, Alexander T., et al. “Systematic Clinician Notification of Incidental Coronary Artery Calcium on Chest CT: The NOTIFY-1 Randomized Clinical Trial.” Circulation, vol. 148, 2023, pp. 1152–1161.


 List
List
